


Comparative Study between three Methods to Evaluate the best Technique for Immediate Implantation at the Lower First Molar Site
Ahmed M. Arnab DDS. OMFS. MSc. PhD, Iyad M. Ghoneim DDS. OMFS. MSc.
Private Oral and Maxillo-Facial Surgeons and Implantologists.
Abstract
Immediate implant placement at fresh extraction lower multirooted molars sites is considered to be very difficult due to a series of site-specific anatomical obstacles. The narrow bone septa between the roots which is usually removed during extraction and drilling. As well, the deviation of the burs while drilling causing the misalignment and lack of bone around implants.
Background and Aim
The unique shape of the lower first molar’s roots “mostly two” in which they are separated by bone, is considered to be one of the most complicated sites for immediate implant placement after extraction. Sometimes when this bone is removed during the extraction process, the area becomes unsuitable for immediate implant placement. A new classification system for molar extraction
sites that describes it based upon the bone availability within the socket for stabilization of an immediately placed implant. Three classification categories which are types A, B, and C. The type A socket, which allows for the implant to be placed completely within the septal bone; the type B socket, which has enough septal bone to stabilize but do not completely surround the implant; and the type C socket, which has little to no septal bone (2). Also, a number of complications could happen after extraction and during implant placement, such as the deviation of the implant to one of the bone sockets, the low values of the ISQ and using small implant diameter. All the aforementioned, could be considered as obstacles for immediate implantation.
The aim of this study is to evaluate three different methods and techniques used in order to achieve proper alignment and high primary stability with good surrounding bony structure in immediate implant placement. And compare the outcomes of the ISQ values among the implants of the three groups and to determine the deviation of the implant to one of the bone sockets in the time of insertion.
Methods and Materials
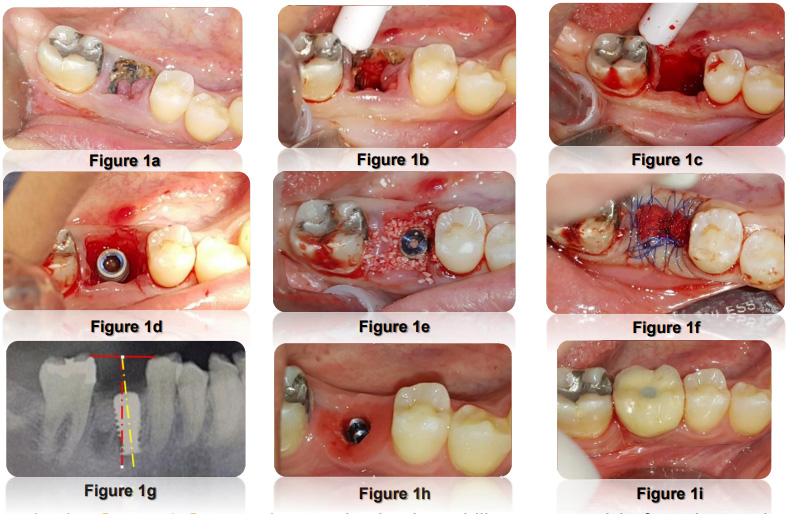
Thirty-Six Lower First Molars were extracted and undergone for immediate implant placement according to a randomized study protocol. The classification of bone septa included in this study was type B. The thirty six teeth were extracted in flapless fashion by sectioning the roots in the bifurcation area and extracted each root atraumatically to save the bony septa as possible. The Specimen was divided into three groups. In the First Group, the tooth was extracted atraumatically and regular implant drills were used into the bone septum at the middle to prepare the
implant site, and then the implant was inserted after the regular osteotomy advised by the implant company surgical protocol. (Figure 1a-i)
In the Second Group, the regular implant drills were used before the tooth was extracted by preparing the upper surface of the tooth, leveling it to the gingival level and then a specific point that fits the mid distance Bucco-Lingual and Mesio-Distal of the tooth to start drilling (Hurzeler Technique). Drilling through the tooth helped guiding the drill into the interseptal bone. After drilling was finished, the roots were extracted and the implant was inserted in accordance to the prepared site (1). (Figure 2a-k)

In the Third Group, the tooth was extracted first and then a point on the middle part of the upper surface for the bony septa was chosen.
Afterwards, drilling has been started using 1.5 mm pilot drill 3 mm longer than the length of the roots. After that DENSAH burs (Versah, LLC 2500 West Argyle Street, Suite 300 Jackson, Michigan 49202) were used in order to achieve the desirable width of the implant. After the preparation of the implant site, the implant was inserted. (Figure 3a-i)

System GmbH (Frankfurt-Eschborn Mergenthaleralle 10-12 D-65750 Eschborn, Germany), which are of a selftapping and platform switching design. The implants were inserted in to the bone 3
to 4 mm longer than the normal roots’ length to enhance the primary stability and were submerged 1 to 2 mm under the buccal bone crest to support the bone level after tooth extraction during healing. Then the Osstell was used to evaluate the ISQ values and the Orthopantomograph to evaluate the axis of the implant and locate any deviation of from the wanted proper alignment. The gap around the thirty-six implants was grafted by OsteoBiol-Gen-Os bone graft (P.za Papa Giovanni XXIII, 2 10094 Giaveno (TO) – Italy) and sealed by Cutanplast-collagen plug (MASCIA BRUNELLI S.P.A.Viale Monza 272 – 20128 Milano – Italy) and sutured in continues fashion. The Orthopantomograph was examined at 3 months and 6 months in order to evaluate the bone healing around the implant. After the healing period (6 months), the ISQ values were taken again before the prosthetic part was applied.
Results
There is a significant statistical difference between the three groups with regard to the ISQ values and deviation values. The ISQ values are excessively low (21-31 ISQ) in the first and second groups (24-48 ISQ). However, the third group values are found to be quite high (63-83 ISQ). The deviation values in the second group are far better than the other groups. After 6 months, the ISQ values are approximately the same between the three groups (68-82 ISQ). The success rate of the thirty-six implant was 100%.

Conclusions
Using DENSAH burs provides great outcomes for ISQ values with a higher primary stability when compared with others groups. These outcomes caused by condensing the bone around the implant and increasing the surface of boneimplant contact. However, it has a little deviation in the implant axis compared with the implants in the second group, but it is much better than the first one (3).
The implants in the second group were in the proper axial line compared with other implants in the first and second groups. Hurzeler technique provides us the wanted axis for drilling without any deviation into any of the bony sockets such in comparison with the implants in the first and the second group were the drilling was done after extraction and the burs deviated into one of the roots’ empty socket (1).
Using osseodensification technique helps in establishing higher primary stability at compromised sites such as the one of the extracted lower first molars as it condenses the bone more around the implant. Long-term follow-up investigation will be documented if the collected data values remain stable over time.
References
- Rebele SF, Zuhr O,Hurzeler MB. Pre-extractive interrradicular implant bed preparation: case presentation of a novel approach to immediate implant placement at multirooted molar sites. Int J Periodontics Restorative Dent. 2013 jan-Feb;33(1):89-96.
- Smith RB, Tarnow DP Classification of Molar extraction sites for immediate Dental Implant Placement: Int J Oral Technical Note Maxillofacial Implants 2013 May-Jun; 28 (3):….911-6.
- Antonello Falco, PhD, DDS. And Michele podaliri Vulpiani, VMD, New Osseodensification Implant Site Preparation Method to Increase Bone Density in Low-Density Bone: In Vivo Evaluation in Sheep, Implant Dent. 2016 Feb;25(1): 24-31.





